Arise Health Plan

- HMO Standard Plans
- HMO High-Deductible Standard Plans
- POS Standard Plans
- POS High-Deductible Standard Plans
| Bronze | Catastrophic¹ | |
|---|---|---|
| Individual Deductiblea specified amount of money that the insured must pay before an insurance company will pay a claim.² | $7,150 | $7,150 |
| CoinsuranceWhat % you pay after your deductible has been met and before your out of pocket max | 0% | 0% |
| Individual Out-of-Pocket MaximumAn out-of-pocket maximum is the most you'll have to pay during a policy period (usually a year) for health care services | $7,150 | $7,150 |
| Teladoc Visit | No charge after deductible | No charge after deductible |
| Retail Clinic Visit | No charge after deductible | No charge after deductible |
| PCP Visit | No charge after deductible | No charge after deductible |
| Specialty Visit | No charge after deductible | No charge after deductible |
| Emergency Room | No charge after deductible | No charge after deductible |
| Outpatient Lab/X-ray | No charge after deductible | No charge after deductible |
| Outpatient Surgery | No charge after deductible | No charge after deductible |
| Hospitalization | No charge after deductible | No charge after deductible |
¹Catastrophic plan includes 3 FREE PCP visits per year. This plan is only available to people under age 30 or who qualify for a hardship exemption from the Federally Facilitated Marketplace. ²Family deductibles and out-of-pocket limits are 2x the individual amounts
| Bronze | |
| Individual Deductiblea specified amount of money that the insured must pay before an insurance company will pay a claim.¹ | $5,500 |
| CoinsuranceWhat % you pay after your deductible has been met and before your out of pocket max | 20% |
| Individual Out-of-Pocket MaximumAn out-of-pocket maximum is the most you'll have to pay during a policy period (usually a year) for health care services¹ | $6,500 |
| Teladoc Visit | 20% after deductible |
| Retail Clinic Visit | 20% after deductible |
| PCP Visit | 20% after deductible |
| Specialty Visit | 20% after deductible |
| Emergency Room | 20% after deductible |
| Outpatient Lab/X-ray | 20% after deductible |
| Outpatient Surgery | 20% after deductible |
| Hospitalization | 20% after deductible |
| Prescription Drugs | Preventative: $0
All others: deductible and coinsurance |
| ¹Family deductibles and out-of-pocket limits are 2x the individual amounts. | |
| Outpatient Facility Fee | 20% after ded. |
| Outpatient Surgery Physician/Surgical Services | 20% after ded. |
| Labs & Diagnostics | 20% after ded. |
| Mental/Behavioral Health & Substance Use Disorder Outpatient Services | 30 |
| Rehabilitation Outpatient Services (Includes Speech, Occupational, Physical Therapy) | 20% after ded. |
| Skilled Nursing Facility | 20% after ded. |
| Pediatric Vision- Routine Eye Exam (1 visit per year) | 100% Covered |
| Pediatric Vision- Eyeglasses (frames, 1 per year) | 100% Covered |
| Pedicatric Vision- Lenses (per pair) | 100% Covered |
| Pharmacy
(Generic / Preferred / Non-preferred / Specialty) |
$10 / $50 / 20% after Rx ded. / 20% after Rx ded. |
| Bronze | ||
| Individual Deductiblea specified amount of money that the insured must pay before an insurance company will pay a claim.¹ | In Network | $7,150 |
| Out of Network | $14,300 | |
| CoinsuranceWhat % you pay after your deductible has been met and before your out of pocket max | In Network | 0% |
| Out of Network | 30% | |
| Individual Out-of-Pocket MaximumAn out-of-pocket maximum is the most you'll have to pay during a policy period (usually a year) for health care services¹ | In Network | $7,150 |
| Out of Network | $20,300 | |
| At Participating Providers² | Teladoc Visit | No charge after deductible |
| Retail Clinic Visit | No charge after deductible | |
| PCP Visit | No charge after deductible | |
| Specialty Visit | No charge after deductible | |
| Emergency Room | No charge after deductible | |
| Outpatient Lab/X-ray | No charge after deductible | |
| Outpatient Surgery | No charge after deductible | |
| Hospitalization | No charge after deductible | |
| Prescription Drugs | Preventative: $0
All others: Ded/Coins |
|
| Individual Deductiblea specified amount of money that the insured must pay before an insurance company will pay a claim.¹ | In Network | $5,500 |
| Out of Network | $11,000 | |
| CoinsuranceWhat % you pay after your deductible has been met and before your out of pocket max | In Network | 20% |
| Out of Network | 50% | |
| Individual Out-of-Pocket MaximumAn out-of-pocket maximum is the most you'll have to pay during a policy period (usually a year) for health care services¹ | In Network | $6,550 |
| Out of Network | $21,000 | |
| At Participating Providers² | Teladoc Visit | No charge after deductible |
| Retail Clinic Visit | No charge after deductible | |
| PCP Visit | No charge after deductible | |
| Specialty Visit | No charge after deductible | |
| Emergency Room | No charge after deductible | |
| Outpatient Lab/X-ray | No charge after deductible | |
| Outpatient Surgery | No charge after deductible | |
| Hospitalization | No charge after deductible | |
| Prescription Drugs | Preventative: $0
All others: 20% after deductible |
¹Family deductibles and out-of-pocket limits are 2x the individual amounts. ²Services performed out of network under the POS plan options are subject to the out-of-network deductible and coinsurance. Out-of-network services are not covered under HMO plan options, except in emergency situations. See policy for details.

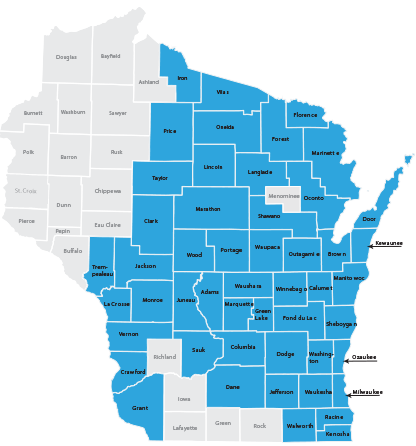
- Adams
- Brown
- Calumet
- Clark
- Columbia
- Crawford
- Dane
- Dodge
- Door
- Florence
- Fond du Lac
- Forest
- Grant
- Green Lake
- Iron
- Jackson
- Jefferson
- Juneau
- Kenosha
- Kewaunee
- La Crosse
- Langlade
- Lincoln
- Manitowoc
- Marathon
- Marinette
- Marquette
- Milwaukee
- Monroe
- Oconto
- Oneida
- Outagamie
- Ozaukee
- Portage
- Price
- Racine
- Sauk
- Shawano
- Sheboygan
- Taylor
- Trempealeau
- Vernon
- Vilas
- Walworth
- Washington
- Waukesha
- Waupaca
- Waushara
- Winnebago
- Wood
Dental Coverage
Optional Dental Coverage
Optional dental coverage includes a variety of routine, basic, and major dental services.
- Annual Maximum Benefit: $1,200 per individual
- Annual Deductible: $50 per individual
- Out-of-pocket savings for all services provided by Delta Dental PPO dentists
- Higher out-of-pocket costs for services provided by non-Delta Dental PPO dentists
- To find a Delta Dental PPO dentist, visit deltadentalwi.com
- Covers dependent children: up to age 26
Summary of Services
| Diagnostic & Preventative Care | You Pay¹ | Frequency |
| Regular cleanings | 20% | 2 per year |
| Routine exams | 20% | 2 per year |
| Bitewing X-rays | 20% | 1 set per year |
| Full-mouth X-rays | 20% | 1 every 5 years |
| Sealants – per tooth | 20% | 1 per lifetime to age 19 |
| Emergency exam | 20% | |
| Restorative Services² | You pay¹ | Frequency |
| Fillings | 50% | 6-month waiting period |
| Simple extractions | 50% | 6-month waiting period |
| Oral surgery | 50% | 12-month waiting period |
| Endodontic services | 50% | 12-month waiting period |
| Periodontic services² | 50% | 12-month waiting period |
| Crowns | 50% | 12-month waiting period |
| Prosthodontics fixed | 50% | 12-month waiting period |
| Prosthodontics removable | 50% | 12-month waiting period |
¹Percent you pay after $50 deductible is met. ²Provides additional Evidence-Based Integrated Care Plan benefits for people with specific medical conditions. Dental Rates
| Age | Adult Rate¹ |
| <30 | $19.46 |
| 30-34 | $22.73 |
| 35-39 | $24.07 |
| 40-44 | $25.96 |
| 45-49 | $28.60 |
| 50-54 | $30.56 |
| 55-59 | $32.43 |
| 60-64 | $32.43 |
| 65+ | $37.09 |
| # of Children | Child Rate¹ |
| 1 | $19.59 |
| 2 | $39.18 |
| 3+ | 67.46 |
Vision Coverage
Summary of Services
| Eye Exam (with dilaton, as necssary) | $5 off routine exam$5 off contact lens exam |
| Complete Pair Eyeglass Purchase¹ | |
| Frames | |
| Any available frame at provider location | 35% off retail price |
| Standard Plastic Lenses | |
| Single Vision | $50 |
| Bifocal | $70 |
| Trifocal | $105 |
| Lens Options | |
| UV Coating | $15 |
| Tint (solid and gradient) | $15 |
| Standard Scratch-Resistant Coating | $15 |
| Standard Polycarbonate | $40 |
| Standard Anti-Reflective Coating | $45 |
| Standard Progressive (add-on to bifocal) | $65 |
| Other Add-ons and Services | 20% off retail price |
| Contact Lenses (discount applies to materials only) | |
| Conventional | 15% off retail price |
| Laser Vision Correction | |
| LASIK or PRK from U.S. Laser Network | 15% off retail price or 5% off promotional price |
| Frequency of use for examination, frames, lenses, or contact lenses unlimited | |
| ¹Frame, lens, and lens option discounts apply only when purchasing a complete pair of eyeglasses. If purchased separately, members receive 20% off the retail price. | |
Contact Us
Phone: (312) 726-6565
Email: [email protected]
Mailing Address
PO Box 11625
Green Bay, WI 54307-1625